Endometriosis
Endometriosis is a disease in which tissue similar to the lining of the uterus grows outside the uterus, causing severe pain and fertility problems. It affects 10-15% women of reproductive age, including two million Polish women. In 96% cases, it reduces fertility, and in half of patients with infertility, it is the main cause of pregnancy problems. Although the exact causes remain unknown, researchers point to hormonal, genetic and immunological factors. Early diagnosis is crucial - the sooner the condition is detected, the better the chances of successful treatment and motherhood. Find out how to recognise the symptoms of endometriosis and what treatments modern medicine offers.

Highlights
- Endometriosis affects 10-15% women of reproductive age, and in 96% cases causes reduced fertility.
- The causes of endometriosis remain unknown - scientists point to hormonal, immunological, genetic and environmental factors.
- Prompt diagnosis is key - the earlier the diagnosis, the better the chances of successful treatment and motherhood.
- In vitro is the most effective treatment for infertility in patients with stage III and IV endometriosis.
What is endometriosis?
Endometriosis is a condition in which tissue similar to the lining of the uterus grows outside the normal location which is the uterine cavity. It can cause severe pelvic pain and make it difficult to get pregnant. Endometriosis can start at the time of first menstruation and last until menopause.
Underlying endometriosis, also known as uterine adenomyosis, is the atypical and abnormal growth of endometrial tissue, or endometrium, in other locations in the body. It begins to appear outside of its proper location, which is the uterine cavity, forming scattered clusters usually within a woman's reproductive organs and the pelvis. Often, foci of endometriosis are located in the caesarean section scar and within the uterine muscle or travel to other organs in the peritoneum, locating in the bladder, intestines and throughout the pelvis. It also happens, although extremely rarely, that endometrial lesions have been found in the lung parenchyma, on the retina, on the skin or even in the brain.


Often, the symptoms of endometriosis that prompt a patient to see a doctor are menstrual cycle disorders and problems getting pregnant.
Despite this wide spectrum of symptoms, endometriosis may not be easy to diagnose, as the symptoms can occur in varying numbers and severity and are often underestimated by patients.
It is only problems with conception that prompt a woman to visit a specialist and take a deeper look at previously downplayed disease symptoms.
Equally common is, that the disease is asymptomatic, and its detection occurs incidentally - during abdominal surgical intervention or during a gynaecological examination.
Endometriosis - causes and aetiology of the condition
Although endometriosis as a condition has been known for almost two hundred years, the exact causes of endometriosis are still unknown. The results of many years of research on endometriosis bring together several different theories, indicating the mechanisms and causes of endometriosis.
It is nowadays believed that a number of immune, hormonal, environmental and genetic factors are responsible for the formation of endometriosis, with an additional influence on the severity and distribution of outbreaks by a number of mechanisms, some of which are still not understood.
Key concepts shedding light on the causes of endometriosis development include:
- transplantation theory (also known as Samson's theory or retrograde menstruation theory) is one of the oldest theories attempting to explain the formation of endometriosis. It was first proposed by Dr Samson in 1920.
According to its tenets, it is believed that during menstruation, in addition to the physiological and normal expulsion of exfoliated endometrium from the uterus, so-called retrograde menstruation also occurs, during which the monthly blood travels upwards through the fallopian tubes to the peritoneal cavity. The endometrial cells, retaining their ability to survive in an environment that is foreign to them, multiply to form foci of disease.
This seems a logical hypothesis, but it does not explain the phenomenon completely. For, according to estimates, retrograde menstruation affects up to 90% women in their reproductive years, and only 10% of them develop endometriosis.
Nor does this theory explain how endometrial cells reach such distant locations as lung tissue, skin or the brain,
- immunological theory turns to immune disorders, pointing to a mechanism whereby, due to immune deficits, the remaining remnants of monthly blood are not removed by the cells of the immune system. Attention is drawn in particular to the increased production of cytokines by macrophages (e.g. overproduction of tumour necrosis factor (TNF) and interleukins). This, often localised, immunological impairment can lead to the survival of endometrial cells in areas that are abnormal for them,
- genetic theory is still a young theory, based mainly on family history. Although a specific gene responsible for the increased risk of endometriosis has still not been identified, a group of genes are mentioned. These include oestrogen, progesterone and androgen receptor genes, the p53 gene and the cytochrome P450 1A1 gene.
Studies on monozygotic twins have confirmed the involvement of these groups of genes and the inheritance process in the development of this disease. It is also noticeable that there is an increased incidence of endometriosis in women whose mothers and sisters also suffer, or have suffered, from it,
- hormonal theory draws attention to the fact that the endometrium growing outside the uterus behaves in exactly the same way as the endometrium inside it. Hence, an excess of oestrogens is considered to be the genesis of the disease, which not only is thought to promote endometrial proliferation, but, above all, causes the cells to survive in locations unfavourable to their development,
- environmental theory draws attention to external factors that may influence endometrial cell hypertrophy and migration. Such factors include the consumption of large amounts of red meat, pollution and a sedentary lifestyle causing declines in immunity, which are associated with the theory of an immune origin of endometriosis, and with an increase in estrogen levels, referred to in the theory of a hormonal origin of the disease.
In addition to the above theories, attention is also drawn to the theory of migration of endometrial cells through the lymphatic and circulatory systems (which could explain the appearance of endometriosis foci in parts of the body that are located distal to the uterus), and the theory of metaplasia (called Waldeyer's theory), according to which healthy endometrial cells transform inside the uterus into pathological cells with different morphological and functional properties and then acquire the ability to move outside the uterine area.
Putting the subject very broadly, we can say that endometriosis is a type of spontaneous transplantation of endometrial cells.
Who is most at risk of endometriosis?
Risk factors can be derived directly from the above concepts of endometriosis formation. The most common risk factors include family history (women with a family history of endometriosis are up to 3 to 10 times more likely to develop the condition) and immune-mediated conditions (i.e. visceral lupus, rheumatoid arthritis or Hashimoto's disease), but it is equally common to see a correlation of endometriosis with factors such as:
- impaired outflow of menstrual blood from the uterus - due to malformations of the uterus (uterine septum, retrogression, uterine or cervical hypertrophy, hymenal hypertrophy and others), in the course of past trauma, infections or surgery,
- early onset of menarche, i.e. the first menstrual bleeding,
- short menstrual cycles (less than 27 days) and associated higher incidence of bleeding,
- childlessness.
Despite the fact that endometriosis is being diagnosed in a growing number of women every year, its causes and risk factors still leave much to be discovered. All the more reason, however, to pay attention to your body and seek specialist help as soon as possible if you have concerns or doubts.
How to diagnose endometriosis?
The diagnosis of endometriosis begins with a medical history taking and a gynaecological examination. The doctor may recommend an ultrasound or magnetic resonance imaging (MRI) scan. According to the latest guidelines of the European Society of Human Reproduction and Embryology (ESHRE), the diagnosis of endometriosis should now be based more on imaging than laparoscopy.
Stages of endometriosis
Endometriosis is a heterogeneous condition and the size and extent of the lesions can vary, as highlighted by the American Society for Reproductive Medicine (ASRM), which has classified the condition into four grades based on the size, number and type of lesions.
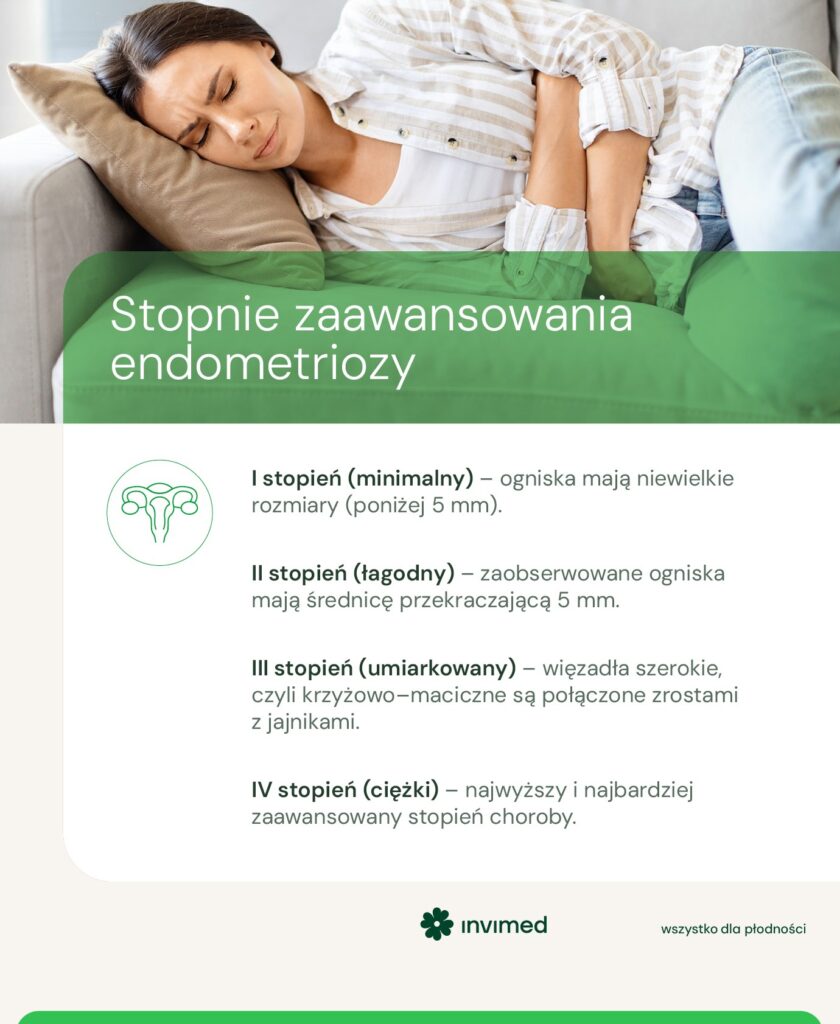
ASRM classification of endometriosis:
- Grade I (minimum) - foci are small in size (less than 5 mm). There may be uninvolved adhesions or free fallopian tube stroma in the ovaries and fallopian tubes,
- Grade II (mild) - The foci observed are more than 5 mm in diameter and the clinical picture may show adhesions between the ovaries and the broad ligaments, in the fallopian tubes, ovaries or in the uterine-ovarian hollow. In some patients, chocolate cysts are present,
- Level III (moderate) - The broad ligaments, or sacro-uterine ligaments, are connected to the ovaries by adhesions. Outbreaks of endometriosis are also seen in the ovarian adhesions and in the uterine-uterine recess,
- Grade IV (severe) - The highest and most advanced stage of the disease. It is characterised by a lack of uterine mobility on palpation and gynaecological examination, and the uterus itself is adherent in posterior tilt to the intestines or severely displaced posteriorly. The bowels are in adhesions with the peritoneum of the uterine recess, with the uterine body or with the uterosacral ligaments. The foci are also located in the cervix, the vagina and may extend beyond the pelvic perimeter.
The insidiousness of endometriosis is that worrying symptoms may not appear at all as the disease progresses. A severe form of endometriosis may be completely asymptomatic, while even small foci can cause pain of considerable severity.
What areas are most commonly affected by endometriosis?
Endometriosis usually first affects areas in the immediate vicinity of the uterus, as well as the uterus itself. As it grows with each successive stage of the disease, endometriosis foci can appear in more and more areas of a woman's body, even reaching completely unexpected nooks and crannies.

In extremely rare cases, endometriosis foci are diagnosed in parts of the body as distant from the uterus as the lungs, retina, brain or skin.
Endometriosis and pregnancy
It is estimated that up to 40-50% women with infertility have endometriosis.
- Endometriosis doesn't have to mean giving up on motherhood - it's important to diagnose it quickly and implement the right treatment - says doctor. Jarosław Kaczyński, gynaecologist-obstetrician, endocrinologist, Medical Director of Invimed Warsaw Mokotów Invimed.
The disease can make it difficult to get pregnant, causing difficulties with fertilisation and embryo implantation. Adhesions, caused by the disease, can cause obstruction of the fallopian tubes, and chronic inflammation has a toxic effect on the ova and the embryo. The disease disrupts hormone secretion by the ovaries, reduces ovarian reserve (i.e. the number and quality of ova), disrupts endometrial function limiting the possibility of embryo implantation and, if implantation does occur, can cause habitual abortions. At a later stage, the disease can lead to a decrease in oocyte quality and abnormal interactions between egg and sperm. Pain during intercourse causes a fear of intercourse and a decrease in libido, which makes couples trying to have a child have less frequent or incomplete intercourse.
The modern approach to treating infertility in a couple struggling with the impossibility of obtaining a pregnancy, in practice means treatment in an in vitro fertilisation programme. Through controlled ovulation stimulation, we obtain several - several follicles containing a mature oocyte. After fertilisation of the oocytes, we monitor the development of the embryos up to day 5/6 in order to cryopreserve them at the blastocyst stage. The embryos thus obtained, can be transferred into the uterine cavity, previously prepared for this in a hormonal therapy dedicated to patients with endometriosis / adenomyosis.
Therapy planned in this way results in a very high pregnancy rate, shortens the waiting time for the desired child and bypasses all those problems in human procreation that a diagnosis of endometriosis brings with it.
If a patient with endometriosis is not currently considering motherhood, it is reasonable to safeguard her oocytes for the future, because in the course of a disease process such as endometriosis, the oocytes undergo accelerated degradation and their quality is lower than the woman's biological age would suggest.
How to treat endometriosis?
In the treatment of endometriosis, the first-line treatment is pharmacotherapy, which aims to reduce pain, restore the endometrium to as normal a state as possible and normalise hormones - especially lowering estrogen levels. If endometriosis is further advanced, laparoscopy, a minimally invasive procedure during which endometrial lesions are removed, is performed. In the case of advanced endometriosis, where the lesions are large or involve multiple organs, it may require surgical treatment.
Other treatments for endometriosis include surgical treatment and combined treatment.
The treatment of endometriosis and the choice of the appropriate method depends primarily on the stage of the disease and the changes occurring, but also the tolerance to pharmacology, the cost of treatment and the woman's plans for future pregnancy and motherhood.
Endometriosis - pharmacological treatment
Pharmacological treatment of endometriosis is aimed at inducing the absence of menstrual bleeding and bringing about hypoestrogenism, which in theory is supposed to prevent the growth of the endometrium and allow the regression of already existing lesions. In practice, pharmacotherapy consists mainly of taking contraceptive drugs, gestagens, as well as drugs that reduce ovarian secretion of oestrogens and gonadotropins secreted by the pituitary gland. Hormonal treatment is usually combined with the administration of non-steroidal anti-inflammatory drugs (NSAIDs), which are mainly used to reduce pain and inflammation within the endometriosis foci.
It should be noted, however, that the contraceptive effect of pharmacotherapy can have a negative impact on the patient's fertility even after therapy has ended, and the passage of time means that the later the diagnosis has occurred, the more difficult it may be to become pregnant later.
The treatment of endometriosis symptoms relies on drugs such as:
- oral contraception It is a first-line therapy, especially in the youngest patients. Its purpose is to reduce or completely eliminate both menstrual pain and pain caused by endometriosis foci. To this end, patients usually take it continuously, without an eight-day break period for the induction of menstruation.
- progestogens have the effect of inhibiting the growth of endometriosis foci or even their complete disappearance. They can be taken orally, intramuscularly or in the form of a hormone-releasing IUD. Side effects of progestogens include weight gain, lowered mood, water retention and irregular bleeding.
- gonadoliberin analogues reduce the secretion of gonadotropins from the pituitary gland. The drug can be taken subcutaneously, intramuscularly or intranasally. Therapy lasts six months; unfortunately, many patients do not opt for it due to the high cost. Side effects of the analogues are mainly hypoestrogenism, which can lead to osteoporosis.
- aromatase inhibitors - These enzymes have an important function in the production of gestagens and oestrogens. They are favoured because their use does not affect bone density and does not cause the risk of osteoporosis.
- non-steroidal anti-inflammatory drugs used for pain relief. They have the advantage of being free of increased side effects and are widely available and low in price.
Pharmacotherapy is aimed at young women who are not yet planning a pregnancy, as well as at women who are already mothers and do not want or foresee a subsequent pregnancy because it delays their efforts to have a child.
Surgery and surgical treatment of endometriosis
The surgical treatment of endometriosis is aimed at releasing adhesions, resecting endometrial foci and tumours and restoring anatomical conditions. It also has a significant impact on symptoms such as infertility and pain.
For this reason, the majority of patients qualified for surgical treatment are women with pain, unresponsive to pharmacotherapy. Direct indications for surgical treatment also include large endometrial cysts (greater than 3 cm), infiltrating other organs (bowel, urinary tract or vaginal-anal septum) and infertility for which other causes have been ruled out during diagnosis.
Two types of surgical treatment of endometriosis can be mentioned:
- Conservative surgical treatment - aims to remove the foci of disease and restore normal mobility and function of the pelvic organs. The treatment should reduce the patient's pain and significantly improve fertility, increasing the chance of natural conception. Conservative surgical treatment is intended to eliminate as many foci as possible and reduce the risk of recurrence. It should be noted that complete removal of foci may be difficult or even impossible. If even the smallest piece of abnormal tissue is left behind, the disease may recur and the previous complaints may persist.
The surgical technique of choice is laparoscopy, as it is less invasive and much safer than laparotomy. It is also associated with fewer complications and a quicker return to full function.
- Radical surgical treatment is usually used in particularly difficult cases where pharmacotherapy and conservative treatment have not had the desired effect. It involves the removal of the uterus together with the adnexa, inducing surgical menopause.
During a laparotomy, the surgeon has a full view inside the abdominal cavity and can therefore remove even those foci that would be difficult or impossible to reach laparoscopically.
For women of childbearing age, this means that they have to be aware of the impossibility of getting pregnant after such an operation, so it has to be a well-considered decision, as the effects of the procedure are irreversible.
Can endometriosis recur?
Even the most varied drug treatment or the most thorough surgery cannot guarantee a complete cure. The treatment undertaken aims to reduce the discomfort, but does not guarantee that the symptoms will not return with the same strength.
The risk of recurrence is significantly lower with appropriately performed surgery than after drug therapy, but neither method is a guarantee of no recurrence.
In general, a correlation can be seen between the severity of the disease before treatment and subsequent recurrence - the higher the degree of endometriosis, the higher the risk of recurrence.
In vitro and endometriosis
In vitro is the method proposed in stage III and IV of the disease, as well as in the case when, despite a small number of lesions, there are additional factors that prevent an attempt at insemination (e.g. fused fallopian tubes). The results of clinical trials indicate that in vitro fertilisation is the most effective form of infertility treatment for patients with endometriosis. The fusion of the sperm with the ovum outside the body eliminates the adverse environmental conditions that accompany endometriosis. Thanks to this, as shown by a study conducted in the USA on the basis of more than 350 000 cycles, in the group of patients in which the only cause of infertility was endometriosis, the birth rate was even higher than in the group of women diagnosed with infertility of another cause.
However, endometriosis worsens the prognosis, due to reduced ovarian reserve, poorer oocyte quality, progesterone resistance or implantation disorders.
It is worth noting that in vitro fertilisation can preserve a woman's fertility for the future. In the event that the operation results in a lower ovarian reserve (due to endometrial cysts of the ovaries, removed during the operation), the patient may benefit from freezing the embryos or oocytes even before the operation, which may increase the chances of pregnancy after the operation.
How to live with endometriosis?
Neither the causes of endometriosis nor the drug or medical procedure that would give 100% a chance of recovery are fully understood.
However, an increasing role is being given to lifestyle and diet in patients with endometriosis. These can effectively influence the quality of life with this disease.
There are increasing claims that an appropriate diet can alleviate symptoms and should be an adjunct to therapy alongside pharmacological and surgical methods. The main aim of diet in the treatment of endometriosis is supposed to be to calm the ongoing inflammation in the body and lower estrogen levels.
Therefore, the diet in endometriosis should be rich in:
- vegetables and fruit that provide antioxidants,
- omega-3 unsaturated fatty acids (oily marine fish and seafood, avocados, olive oil),
- products containing cysteine and glutathione (white meat, tuna, beans, lentils and other legumes),
- products containing lycopene (tomatoes) and beta carotene (carrots, beetroots, peppers).
For more information on a proper diet in endometriosis, see the e-book prepared by the Invimed team.
It contains both general dietary information and ready-made recipes.
Free e-book: Dietary relief for endometriosis
The right diet can reduce pain, improve immune function and support the endocrine system.
Appropriate physical activity can also support the treatment of endometriosis. Moderate-intensity exercise, while supporting the immune system, has an anti-inflammatory effect and, in addition, has the power to regulate hormones - primarily insulin and oestrogen, which are, after all, crucial in the treatment of endometriosis.
In addition, movement oxygenates internal organs and joints and improves the mobility of the latter, raises endorphin levels and helps the nervous system to recover more effectively and cope with chronic pain.
Studies show that regular moderate to high-intensity exercise significantly improves the quality of life of patients with endometriosis. However, in order for the improvement to be noticeable, it is necessary to exercise at least three times a week for 30 minutes.
Recommended activities include:
- yoga, pilates and stretching,
- swimming and jogging,
- fitness training and dance classes.
But also any other form of movement that makes the patient feel better.
Also invaluable are all breathing exercises and relaxation techniques, which additionally help to combat stress, which has its part in exacerbating inflammatory processes. Also in endometriosis.
Among the activities that are not recommended are all sports that can cause tension and hypoxia in the pelvic and abdominal area, which can exacerbate symptoms. These include strength, interval and crossfit training, combat sports, tennis and all exercises focused on increased abdominal muscle work.
Every woman is different and has different needs, so if in doubt, you can seek the help of a physiotherapist to help tailor the exercises to your needs. It is also worth observing your body and the signals coming from it - both during and after exercise.
According to Swiss researchers, women suffering from endometriosis may experience chronic fatigue up to twice as often as their healthy counterparts. This exhaustion may be a consequence of chronic inflammation, putting a strain on the immune system and resulting in fatigue. Therefore, just as important to support treatment as the aforementioned diet and physical activity is ensuring adequate rest and avoiding stress whenever possible.
Endometriosis is a chronic and severe disease, despite the fact that it often does not give clear symptoms and its detection remains a matter of chance. Although the disease mainly affects women of childbearing age, it can also occur in young girls.
Diagnosis is not straightforward, but failure to do so can result in delayed treatment and associated progression of the disease, so when endometriosis is suspected it is worth referring to a specialist for correct diagnosis.
Author text




- Spaczyński, R. Z., Kotarski, J., Bidziński, M., Drosdzol-Cop, A., Jach, R., Paszkowski, T., ... & Zawiejska, A. (2013). Position of the expert group of the Polish Gynecological Society in the treatment of endometriosis. Polish Gynaecology, 84(11), 871-879. https://journals.viamedica.pl/ginekologia_polska/article/download/46120/32910
- Endometriosis Institute Wrocław. (2024). By treating endometriosis, we restore women's fertility. https://instytutendometriozy.pl/leczac-endometrioze-przywracamy-kobietom-plodnosc/
Frequently asked questions - FAQs?
Yes, a predisposition to endometriosis can be hereditary. Women whose mothers or sisters suffered from endometriosis have a 3-10 times higher risk of developing the disease. Studies on monozygotic twins have confirmed the involvement of genetic factors in the development of the disease.
After treatment of endometriosis, regular follow-ups with a gynaecologist every 6-12 months are recommended. The frequency depends on the stage of the disease and the therapy used. Check-ups allow early detection of a possible relapse and prompt implementation of appropriate treatment.
Yes, chronic stress can exacerbate endometriosis symptoms by exacerbating inflammatory processes in the body. Stress also affects the endocrine and immune systems, which can worsen the course of the disease. Therefore, it is important to use relaxation techniques and take care to rest.
The cost of endometriosis treatment varies widely. Basic tests and pharmacotherapy can be reimbursed by the National Health Service. Additional varying costs: private laparoscopic procedures, gonadoliberin analogues and IVF treatment.
The medical information presented should be considered as general guidelines and does not replace the individual judgement of the doctor regarding the medical management of each patient. The doctor, after a thorough examination of the patient's condition, determines the extent and frequency of diagnostic tests and/or therapeutic procedures, taking into account specific medical indications. All medical decisions are made in full consultation with the patient.
Author of the article
Invimed editorial team - we serve patients by solving their fertility problems. We use world medical knowledge, state-of-the-art technology and treatment methods. We are here to make dreams of parenthood come true. The smiles on the faces of happy parents give meaning to our work.
See all articles →